Stress incontinence is urinary leakage that occurs at times of increased abdominal pressure or strain. It can occur when laughing, coughing, lifting weights or even just walking, depending on its severity.
What causes it?
The female bladder is supported by the pelvic floor muscles and various the committee's attachments. If there is any disruption to the system, either by destruction stretching of the ligaments or failure of the sink the mechanism then urine can leak during times of strain.
Urethral hypermobility
This occurs when the ligaments supporting the urethra and bladder neck are stretched or disrupted. This allows excessive movement of the urethra under abdominal strain that subsequently results in you and league.
Intrinsic sphincter defect
This occurs when the urethral sphincter lacks the ability to close completely, therefore cannot provide a waterproof seal to prevent urinary leakage.
How is it investigated?
You may require some or all of the following tests:
-
Urine culture.
-
You may be asked to complete a bladder diary.
-
Pad test – this involves weighing an incontinence pad that has been worn either a single hour or a whole day. This allows calculation of the amount of urine loss.
-
Urodynamic assessment.
How is it treated?
There are a number of treatments for stress incontinence in women. The majority of women will certainly respond to one or a combination of the therapies.
Lifestyle changes
-
Weight loss can prove beneficial in improving the severity of stress incontinence.
-
Pelvic floor exercises – these can be done by oneself or under the supervision of physiotherapist with an interest in incontinence.
-
Weighted vaginal cones – these can be used to increase the intensity of pelvic floor exercises. This is the equivalent of going to the gym.
-
Biofeedback – various devices are now available to help measure the degree of pelvic floor contraction and hence give feedback to allow a woman to judge the effectiveness of the exercise regime.
Electromagnetic stimulation

There are various models of treatment chairs that deliver deep electromagnetic stimulation to the public for musculature. These further enhance the effect of pelvic floor exercises as they guarantee the correct muscle groups are contracted.
Surgical Options
Bulking Agents
The injection of a bonding agent into the urethra helps prevent incontinence by opposing the walls of urethra. This bulking aids the sphincter muscle to remain closed under strain. Most bulking agents these days are water-based, large molecule compounds that can simulate normal tissue.
They can be used alone or as as an additional therapy to support other treatments such as a mid urethral sling
Mid-Urethral Sling
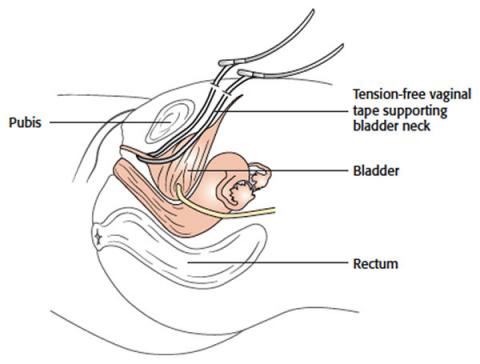
As one of the main contributing factors to female stress incontinence is the excess mobility of the urethra due to stretching or breaking of the pupa urethral ligaments. Re-constructing these ligaments using a tension free vaginal tape (TVT), positioned in the mid urethra, has proven to be a successful and reliable treatment option.
The procedure typically involves an overnight stay in hospital and a rapid recovery - though the patient needs to avoid activities that involve abdominal straining for a period of six weeks after discharge. There are two common approaches, and either the retropubic or trans-obturator technique will be utilised.
Fascial Sling
Occasionally, in complicated cases a patient’s rectus fascia is utilised to form a sling under the urethra at the level of the bladder neck. This is a much larger procedure from the patient's point of view as it involves a longer hospital stay, moderately large abdominal incision and longer recovery period.
It is commonly used when synthetic materials are contra-indicated, or when the patient has had previous surgical options that have failed.