What is kidney cancer?
A cancer is an abnormal growth in an organ of the body. The most common type of kidney cancer is known as a renal cell carcinoma (RCC). This is a solid tumour of the “meat” of the kidney.
There are other, less common tumours of the kidney such as transitional cell carcinoma (TCC) – this is a cancer of the lining of the kidney. There are also cancers that have spread from elsewhere such as lymphoma, sarcoma and other metastatic cancers.
Who gets kidney cancer?
Kidney cancer accounts for approximately 3% of all adult cancers. It is more common with age – the majority of people are aged between 40 & 60 years. Men are affected 2-3 times more frequently than women.
What are the causes of RCC?
Whilst there are no specific causes known for RCC there has been evidence showing a genetic tendency to develop RCC in people who have certain genes, a family history does not increase the risk particularly. There are two genetic disease that increase the risk:
-
Von Hippel-Lindau disease.
-
Tuberous sclerosis.
There is also an increased incidence of RCC in patients with the following:
-
Horseshoe kidneys.
-
Adult polycystic kidney disease.
-
Dialysis patients who develop kidney cysts.
What are the symptoms?
The vast majority of kidney tumours are found incidentally when a person is having a scan (ultrasound or CT) for some other reason. The tumour itself is causing no symptoms whatsoever, so the discovery is truly accidental.
If they do cause symptoms the most common is:
-
Haematuria – blood in the urine, with or without clots.
After bleeding most symptoms are, in fact, quite rare, but include:
-
Loin pain (back pain).
-
A lump you can feel in the abdomen.
-
Weight loss.
-
Fatigue.
-
Night sweats.
-
Sudden appearance of a varicocele (varicose veins to the testis).
-
Pain in the bones.
-
Shortness of breath.
What tests are needed?
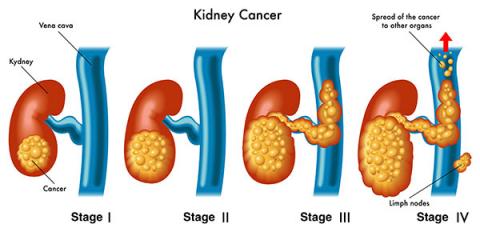
The most important test is often the way the kidney cancer is discovered in the first place. Tests are also important to determine the staging of the tumour, that is:
-
Size.
-
Position in the kidney.
-
Has it spread beyond the kidney.
-
Has it spread to other parts of the body.
Not all patients will need all tests, but you may need:
CT Scan
This is the definitive test for a kidney cancer. It outlines the size and position of the tumour within the kidney, as well as any extension it may have into the blood vessels or lymph nodes. It also has the advantage in that it outlines the other abdominal organs and allows proper planning of any surgery that may be required.
Ultrasound
An ultrasound is often the first test organized when a person presents with haematuria (blood in the urine). It can readily distinguish between a solid mass and a cyst (which is fluid-filled).
Renal Scan
This is a nuclear medicine scan that is occasionally required to help determine the relative function in both kidneys. This is important if there is some impairment to normal kidney function, and there is the possibility that one kidney may need to be removed.
Chest X-ray
The most common area that kidney cancer spreads to is the lung so it is usual to check to make sure a kidney cancer has not metastasized there.
Bone Scan
This test is done to look for spread of cancer to the bones, which will turn up as a dark spot on the scan.
Cystoscopy
This is a telescope inspection of the bladder. It is usually performed as blood in the urine is often the presenting symptom, and this test is the only way to make sure there are no tumours in the bladder.
Blood Tests
These are usually performed to look for anaemia, as well as to check the renal function and exclude other biochemical abnormalities that occasionally are associated with kidney cancer.
Kidney Biopsy
Until quite recently a kidney biopsy was not thought to be of use if kidney cancer was suspected. There have been improvements in imaging & biopsy techniques that have resulted in the more frequent use of kidney biopsy, as part of the management plan in treating kidney cancer.
A kidney biopsy is a small tissue sample obtained by passing a special needle through the back into the tumour in the kidney. It is performed under X-ray control – most often CT scan, but occasionally ultrasound.
It is more likely to be performed in the following circumstances:
-
There is a suspicion of lymphoma.
-
There is doubt whether the mass is a cancer or not.
-
If there is a suspicion the tumour may be a cancer from another part of the body that has spread to the kidney.
How is kidney cancer treated?
The treatment options for RCC (kidney cancer) vary according to the requirements of each individual patient. Options include:
Observation
Not all kidney cancers need to be surgically removed. The risk of a small cancer (<3cm) spreading to other organs is small (1% – 2%). Therefore, it is reasonable to observe such small cancers in some patients, especially those who are frail or elderly.
Surgery
Removal of the kidney cancer remains the main treatment option. There are a number of surgical options depending on the size, position and extent of the tumour.
Radical Nephrectomy
This is a major operation where the kidney and the major blood vessels are exposed to allow large tumours that may have extended into the renal veins and beyond to be completely removed. Sometimes the tumour thrombus can extend up the Inferior Vena Cava (the main abdominal vein) all the way to the heart.
Laparoscopic Nephrectomy
This is the “key-hole surgery” option to remove the kidney. Techniques and skills have improved to the extent that this is the most commonly performed technique to remove the kidney.
Partial Nephrectomy
In this surgical option only the kidney tumour is removed. If the tumour is small enough, this has the advantage in that it preserves more renal tissue and is less likely to affect total renal function. It can be performed in either an open fashion (traditional incision) or laparoscopic technique (key-hole). It does have a slightly higher complication rate that your surgeon will discuss with you.
Targeted Therapy
If the tumour is small enough, there has been some experimental work using minimally invasive techniques to treat the kidney cancer alone. This has the advantage of minimal recovery time and maximum preservation of renal tissue. Either radiofrequency energy or cryotherapy (intense cold) is used. There is much excitement on this front and both techniques are available, but they should be regarded as experimental until more data has been collected.