Stress incontinence occurs when urine leaks from the bladder will during times of increased abdominal pressure. This occurs during such activities such as coughing, laughing, exercise and lifting heavy weights. Incontinence of this type is much less common in men as not only is there a urinary sphincter to act as the 'is that mechanism' is, but the prostate is usually present at acts as a backstop to dissipate increased pressure
What causes it?
The most common cause is damage to the urinary sphincter that occurs during the complete removal of the prostate as treatment for prostate cancer. After the surgery 50-60% of men will experience some form of temporary incontinence, 5-10% will have persistent incontinence and 1-2% will have severe incontinence.
Other causes include:
-
Pelvic trauma.
-
CVA (stroke).
-
TURP - very rare less than 0.5%.
-
Unknown.
What tests may be required?
Some or all of the test listed below may be required to investigate and experiencing incontinence. It is important to know the exact nature and severity of the incontinence in order to plan appropriate therapy.
Tests include:
-
Bladder diary.
-
Pad tests.
-
Urodynamic assessment.
-
Cystoscopy.
What are the treatment options?
Conservative Options
Pelvic Floor Exercises
Pamphlets are readily available with instructions on how to perform pelvic floor exercises in an effective manner. There should be initiated in a like manner with a gradual increase in intensity. Supervision by a trained physiotherapist with an interest in this area has been shown to significantly improve results.
Incontinence Devices
The practice nurse can readily direct you to the appropriate pads and other devices that can help keep you come to be dry.
Lifestyle Changes
Modifying the amount and type of fluid intake can make a difference to the degree of incontinence. For example, decreasing the daily coffee and take all the timing of alcohol can improve social situation.
Surgical Options
Bulking Agents
Urethral bulking agents are the most minimally invasive surgical option, and were viewed with great enthusiasm when they were first introduced. When used as a primary therapy long-term success was very disappointing, except in a few very select patients. They are best used as a supportive treatment to the sling procedures
Male Sling Procedures
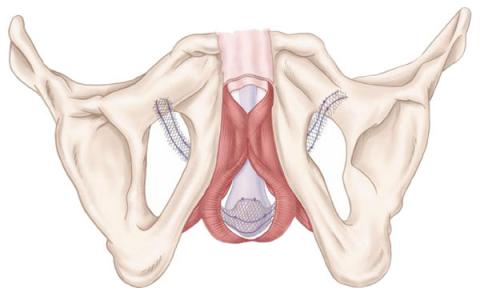
The concept of a male sling is a relatively new one compared to the options available for women. They have however, proven to be a reliable and less invasive treatment option for the appropriate man.
Whilst there are a number of different slings presently available they do share a number of characteristics. They are usually positioned through an incision in the perineum (the area between the anus on the scrotum), adjusted intra-operatively and involve an overnight stay in hospital. There is a need to avoid excessive abdominal straining for 6-8 weeks post operatively.
Artificial Urinary Sphincter
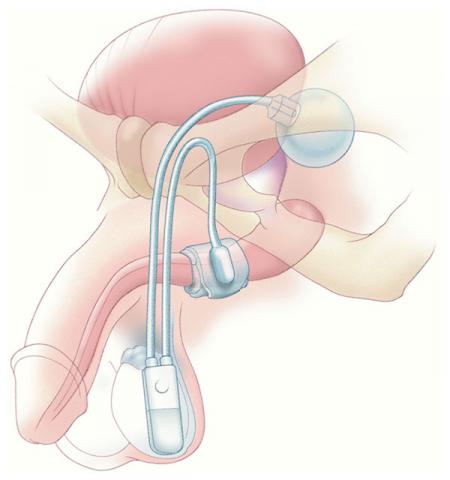
As the name implies this is a device or prosthesis that replaces the damaged urinary sphincter. They are regarded as the gold standard therapy for the treatment of male incontinence. They are highly successful and have been proven to be a long-term solution to the problem.
Whilst there are a number of artificial sphincters more recently released, they have no long-term data as compared to the AMS 800, which has been implanted for more than 30 years now. It consists of three components:
-
The pump – which is implanted in the scrotum
-
The cuff – an inflatable surrounding the urethra that mimics the sphincter and is controlled by the pump
-
The reservoir – which is implanted in the abdomen, controls the pressure generated by the cuff
The operation itself involves an overnight stay in hospital, and most men make a rapid recovery and return to normal activities within a short period. The device is usually activated one month after discharge.